Total Knee Replacement
Knee replacement surgery (arthroplasty) is a common operation that involves replacing a damaged, worn or diseased knee with an artificial joint.
Why do I need a Total Knee Replacement?
Total knee replacement surgery is usually necessary when the knee joint is worn or damaged so that your mobility is reduced and you are in pain even while resting.
The most common reason for knee replacement surgery is osteoarthritis. Other health conditions that cause knee damage include:
- rheumatoid arthritis
- haemophilia
- gout
- disorders that cause unusual bone growth
- death of bone in the knee joint following blood supply problems
- knee injury
- knee deformity with pain and loss of cartilage
Who is offered knee replacement surgery?
A knee replacement is major surgery, so is normally only recommended if other treatments, such as physiotherapy or steroid injections, have not reduced pain or improved mobility.
You may be offered knee replacement surgery if:
- you have severe pain, swelling and stiffness in your knee joint and your mobility is reduced
- your knee pain is so severe that it interferes with your quality of life and sleep
- everyday tasks, such as shopping or getting out of the bath, are difficult or impossible
- you're feeling depressed because of the pain and lack of mobility
- you cannot work or have a social life
You'll also need to be well enough to cope with both a major operation and the rehabilitation afterwards.
What happens during the surgery?
A knee replacement is a major operation and usually takes approximately two hours.
During a total knee replacement operation:
- The worn surfaces at the bottom end of the thigh bone (femur) and the top end of the shin bone (tibia) are removed.
- The surfaces are covered with metal implants fixed in place with bone cement.
- A smooth plastic insert is fixed to the top of the tibial implant. This ensures that the two surfaces glide smoothly together.
- Sometimes the underside of the kneecap (patella) is also re-surfaced with plastic
- The layers of soft tissue, muscle and skin are repaired and stitchedback together.
You are usually in hospital for one to two nights. You should be prepared to work hard at the exercises given to you by the therapy staff. Most patients tell us that they are pleased with the result of their knee replacement. Some, however, are less satisfied either because acomplication has arisen or their expectations are too high.
Benefits of a Knee Replacement
The aim of a knee replacement is to reduce pain and improve mobility. About 90% of people having a knee replacement rate the result themselves as ‘good’ or ‘excellent’.
Risks
The vast majority of patients make a rapid recovery after knee replacement operations and experience no serious problems. However, it is important you understand that a knee replacement is a major operation and that complications can occur.
General surgical risks
Thromboses and emboli (blood clots)
Blood clots in the leg veins (deep vein thrombosis) and blood clots on the lungs (pulmonary embolus) are a risk associated with joint replacement surgery. The simplest way of reducing this risk is early mobilisation (exercises and walking). Whilst in hospital you will also be prescribed blood thinning treatment, usually in the form of injections, to reduce the risk of clot formation. Patients already receiving anti-coagulant therapy will be assessed andadvised accordingly.
Urinary problems
Some patients, particularly those who may have previously experienced difficulty passing water, may sometimes need a catheter to be inserted into the bladder prior to or after the operation. There is a small risk of temporary incontinence; particularly in women, following surgery. Except in certain circumstances, this should be removed the morning after
surgery. You will be asked to complete a questionnaire about your urinary habits at your pre-operative assessment. This will help identify any patients that may experience urinary problems after the operation.
Transfusion
Blood transfusion following knee replacements is rarely needed. If your blood count is very low or if you are showing symptoms of anaemia (low blood count), the team looking after you may recommend a blood transfusion.
Superficial Infection
You will not be discharged from hospital unless the appearance of the wound is satisfactory. Where possible, the dressing will stay on until the removal of your clips or stitches.
Deep Infection
A deep infection of the joint most often starts when bacteria gain access to the tissues at the time of surgery and great lengths are taken in theatre to reduce the risks of this happening. Operations are carried out in an ultraclean air theatre and sterile clothing is worn by the surgical team. You will be given preventative antibiotics at the time of surgery.
Despite all the precautions taken, infections can still occur. An early deep infection (within the first six weeks) may rarely occur and this would require a further operation to clean the joint replacement. Occasionally, it would be necessary to take out the joint replacement to resolve the infection. It is likely you would require a course of antibiotics.
An infection can occur at any stage in the life of a knee replacement. The reason for this is that any infection in the body can circulate in the blood and settle on the surface of the new knee joint. Once there it forms its own environment, or ‘bio-film’, which makes it difficult to treat with antibiotics alone. Although the symptoms of infection can often be suppressed with antibiotics the only way to eliminate this deep infection is to remove the artificial implant as described above.
Remember infection is a serious complication. Call 0121 812 3312 between 8am and 4pm Monday - Friday (excluding bank holidays) if you have any of the following symptoms of infection relating to your surgical wound:
- Redness / inflammation / heat
- Pain / hardness
- Discharge from your wound
- Wound gaping
If you have any symptoms that you are concerned about and you require urgent, non-emergency advice contact 111. For all other Medical Emergencies please call 999.
For non-wound infection related queries e.g., follow-up appointments/ dressings / stockings/ sutures / clip removal, please call the discharging ward for advice.
Bruising
It is common to see bruising around the knee in the days after surgery and, occasionally, this bruising will extend down the leg, sometimes into the foot.
Swelling
It is likely that your knee and lower leg will swell. This is a normal response to surgery. It may be many months before this settles. Occasionally, the knee will always remain slightly larger than a normal joint. Some warmth around the knee is another common occurrence and is due to increased blood flow through the tissues during healing. Again, this may
take months to settle. You should continue to do the exercises detailed in this book even if your knee is swollen. Walking can help reduce the swelling, but standing unnecessarily should be avoided.
Using ice can be helpful in reducing swelling and pain but is not appropriate for everyone. Please be guided by your Physiotherapist. You should also aim to elevate the leg for 20 – 30 minutes regularly throughout the day.
Medical Problems
Complications such as heart attack, stroke or death can occur after knee replacement as with other forms of major surgery. These complications are rare and the anaesthetist will not allow the operation to proceed if it is felt that the risks are significantly higher than normal. In this circumstance, it may be that you are sent for further tests or treatment prior to surgery being performed.
Fat embolism
This is rare and is caused by the fat within the bones (marrow) travelling up into your lungs at the time of surgery and causing breathing problems. Although this can be serious it is most commonly treated with extra oxygen therapy.
Specific risks
Stiffness and range of movement:
Most people are delighted with their knee replacement. Some people describe aching or stiffness in the joint or have a limp which does not improve. Sometimes the knee may be unstable. It is vital to follow your rehabilitation programme to achieve the best possible outcome. It can take months to gain a good range of movement. The range achieved varies from person to person. This is due to many factors including:
- Your general health before the operation
- The knee range of movement before the operation
- Your weight
- Any post-operative complications
Fractures
Very rarely, fractures (breaks) of the bone can occur during surgery. These are almost always identified during surgery or on the x-ray taken after surgery. Occasionally this requires further surgery, or you will be asked to reduce your activities for several weeks to allow the fracture to heal.
Nerve Damage
Very occasionally one of the nerves that run past the knee can be damaged during the operation. This can cause footdrop, or paralysis of other muscles in the leg. Although the nerve often recovers over a period of months, the paralysis can persist. The skin around either side of the knee can feel numb after the operation – this is normal. The feeling in the skin may or may not recover but knee function will not be adversely affected.
Blood vessel injury
This is extremely rare but serious. It can sometimes be repaired by a vascular surgeon if needed.
Need for further surgery
In the event of a complication, you may require further procedures such as a manipulation of a stiff knee, a washout, or a revision procedure.
What will happen before surgery?
You will go through the Pre-Operative Assesment Clinic (POAC), this will provide you with the opportunity to discuss the medical, nursing and therapy requirements needed to help you plan for your admission to hospital and discharge following surgery. At the POAC your medical fitness for an anaesthetic will be assessed and any tests required organised.
All patients are screened for MRSA during their Pre-Assessment Clinic appointment. If you are found to be a carrier of MRSA you will be given treatment prior to your operation.
Please inform the nurse if you have been diagnosed in the past with MRSA, C-Diff, VRE, CPE or CJD. Or if you have received treatment in a hospital in this country or abroad, within the last 12 months.
Anaesthetic during surgery
There are two main types of anaesthesia, general anaesthesia and local anaesthesia. They are often combined.
General anaesthesia
It is uncommon for general anaesthesia alone to be used for knee surgery. It is usually combined with a spinal anaesthetic or nerve block. On occasion a deep sedation technique may be used instead of a general anaesthetic. A general anaesthetic is a combination of drugs, which are given to make you completely unconscious. During a general anaesthetic you do not feel anything and will not be aware of what is going on around you. Modern general anaesthetic is very safe. There are some common side effects and some less common side effects:
Common side affects
- Sore throat
- Feeling sick
- Shivering
- Headache
Less common side affects
- Chest infection
- Muscle pain
- Damage to the teeth, lips or eyes
- Excessive drowsiness
Serious complications related to general anaesthesia are rare but include life threatening allergy to drugs, breathing difficulties and cardiac issues such as heart attack and stroke.
Local anaesthesia
Local anaesthetics are drugs that have a numbing effect. They stop you feeling pain and other sensations in part of your body but on their own do not cause any loss of consciousness. Types include the following:
1. Spinal anaesthetic
- Local anaesthetic is injected near to the nerves in your back
- You go numb from the waist downwards
- You feel no pain but you remain conscious
- If you prefer, you can also have drugs that make you feel sleepy and relaxed (sedation). You are likely to have little memory of the time during which you have been given sedation
2. Epidural
This is similar to a spinal anaesthetic. It involves inserting a very fine plastic tube, through which the local anaesthetic is given. It can be used to continue pain relief for several days after your surgery.
Pain control after surgery
Pain following your knee operation is inevitable. We aim for your pain to be at an acceptable level to allow you to move around after your surgery and recover. Pain control is an essential part of your care The nurses and acute pain team are able to give you advice and support. Pain relief is available in different forms and strengths. If you need support, please ask a member of our team for help.
Oral medication
When you are able to drink and eat then you may take your painkillers by mouth. Most patients will need to take painkilling medication regularly after surgery to keep their discomfort to a minimum.
Local anaesthetic
Most patients will receive a spinal anaesthetic and will have long-acting pain killers added to this injection. This can provide very effective pain relief for up to 24 hours after the operation. Injecting local anaesthetic drugs close to the nerves going to the knee, the spinal region or the operation site blocks painful messages from being sent to the brain. The Anaesthetist will discuss this with you in further detail.
What happens on the day of surgery?
The anaesthetist and a member of the surgical team will visit you before surgery. The anaesthetist will explain the anaesthetic and methods of pain control. You will have the opportunity to ask any further questions. They will also discuss your consent again prior to surgery. A member of the surgical team will draw an arrow on your leg to ensure
the correct side is operated on.
When it is time for your operation, one of our team will take you to the changing room. They will go through a series of safety checks and then one of our theatre team will take over your care.
When you have been anaesthetised, you will be taken to the operating theatre. While you are asleep the anaesthetist will remain with you at all times, monitoring to ensure you are safe. If you are awake or under light sedation, you will be aware at times of some noises and vibrations. The anaesthetist will be there at all times to reassure you.
What to expect after surgery
The operation to replace your knee takes approximately two hours. At the end of the surgery, the anaesthetist will wake you up and take you to the recovery area. You may find several items in place to help your recovery. An oxygen mask over your mouth and nose helps your breathing. The drip in your arm should be removed once you are tolerating food and drinks. Your pain control will be established and your vital signs monitored. Once you are fully awake you will then return to the ward.
Once back on the ward you will be given regular pain relief by the nursing staff in the form of an injection or tablet as required. Observations including blood pressure, pulse, respiration rate, oxygen levels and temperature will be recorded. Your skin will be checked and our team will encourage you to change your position regularly to prevent pressure sores.
You may experience some significant discomfort following surgery. You will be given regular painkillers, so you are able to do exercises and move your new knee. You should take the pain medication you have been prescribed whether you are in immediate pain or not. Painkillers include paracetamol, ibuprofen-type drugs (non-steroidal anti-inflammatory drugs) and morphine-like drugs (opioids). Initially, you will need strong painkillers to help you to move. We will give you strong painkillers for one or two days after your surgery. Please remember to let the doctors and nurses know if your pain is not controlled or above or if the pain stops you doing your exercises. We may need to alter or increase your painkillers.
Please don’t be afraid to ask if you need support managing your pain.
The consultant who operated on you will also visit you to review your progress.
The physiotherapist will continue with your exercises and progress your mobility with a walking frame or sticks/elbow crutches
Preparing for home
- You will be taught how to go up and down stairs
- You will be encouraged to walk with sticks or elbow crutches independently
- You will be shown how to give the blood thinner injection
- Your wound will be checked
- When you have achieved all of your discharge goals you will move to the discharge lounge to enable our discharge nurses to explain all of your medication, your discharge paperwork and wait for your family/friend to pick you up
Physiotherapy
After your operation you will be encouraged to be as independent as possible. This is achieved by starting your rehabilitation within a few hours of your operation.
Back at home
Your mobility will be assessed by the Physiotherapy team on the ward, and again if you are seen by ROCS (Royal Orthopaedic Community Scheme), and at your out-patient physiotherapy appointment.
We advise you to continue to use both sticks (or crutches) initially on discharge. When you feel safe and able to walk without a limp, you can progress to one stick indoors, but continue to use both sticks outdoors at this stage. You should do this as you may become very tired, walk with a limp due to muscle weakness, or come across obstacles such as kerbs, broken pavements, crowds etc.
When walking with one stick remember to hold your stick in the opposite hand to the side of your operation. If you are not allowed to take all your weight on your operated leg you will have been provided with appropriate walking aids by the physiotherapist and advised how to progress.
General wellbeing
- It is not unusual to feel tired and your sleep patterns may take a while to return to normal. Remember to have a rest on the bed every afternoon for an hour to reduce swelling in your legs and feet
- Your appetite as well as your bowel habits may take a while to recover. Make sure you drink plenty of fluids and try to eat a healthy balanced diet
- Try not to feel frustrated at not being able to do all the things you want straight away. Increase your activity levels gradually. Start with short distances around the house and garden in the first 2 weeks then increase as you feel able
- Avoid tight clothing including belts and tight underwear. Loose garments are generally more comfortable and are a lot easier to put on
Medication
- It is important that you continue to take all your medication as instructed
- You will have been given a supply of painkillers to take home. Continue to take these as directed until you no longer feel that you need them. Remember your pain should be controlled enough to allow you to move about comfortably and to be able to practice the exercises to strengthen your knee
- You may have been given tablets or injections to administer to thin your blood. It is important that you continue with these as directed
Stockings
- If you have been told to wear your AES or ‘Anti-Embolic’ stockings at home, apart from 30 minutes each day, these must be worn day and night for six weeks following your operation
Going to the toilet
For the first two weeks after surgery it is very common for bowel movements to become irregular. This can be due to the effect of analgesia combined with inactivity and a change of routine. This will resolve itself as you get back into your usual routine at home. However, you can help yourself by eating high fibre foods such as fruit, vegetables and wholemeal bread. If necessary, try taking a mild laxative for a few days until you return to your normal routine. If you need any further advice regarding your diet, please do not hesitate to ask.
Washing and dressing
- You may use a shower when you feel safe to do so. Please do not have a bath for six weeks
- When dressing, sit on the side of the bed or in a suitable chair. This will help your balance
- Collect all the clothes you intend to wear and put them on the bed next to you before you start
- Always dress your operated leg first and undress it last
Driving
Most patients are instructed not to drive for six weeks after their surgery, but your consultant will advise you on this. Make sure you can reach and use the pedals without discomfort. Have a trial run without the engine on. Try out all controls and go through the emergency stop procedure. Start with short journeys and when you do a long trip stop regularly to get out and stand up and stretch. Please be aware that if you drive soon after your surgery and have an accident, insurers may consider you liable for damage. It is advised that you check with your insurance company first, before driving.
Sleeping
Changes in routine and restricted movement can cause difficulty in sleeping. Some people are awakened by the discomfort caused by sudden movement. If this happens, you may wish to take a painkiller to help you sleep.
Safety and avoiding falls
- Pick up loose rugs, and tack down loose carpeting. Cover slippery surfaces with carpets that are firmly anchored to the floor or that have non-skid backs
- Be aware of all floor hazards such as pets, small objects or uneven surfaces
- Provide good lighting throughout
- Keep extension cords and telephone cords out of pathways. DO NOT run wires under rugs, this is a fire hazard
- DO NOT wear open-toe slippers or shoes without backs. They do not provide adequate support and can lead to slips and falls
- Sit in chairs with arms. It makes it easier to get up
- Rise slowly from either a sitting or lying position in order not to get light-headed
- DO NOT lift heavy objects for the first three months
- Stop and think. Use good judgement
Sitting
Choose a chair that is comfortable for you. Chair arms will help you get up and down safely in the first few weeks after surgery. To sit down and stand up safely, walk to your chair, slowly step back until you feel the back of your legs touching the seat. If you are using crutches, take your arms out of them and hold the handles in one hand before sitting.
To get up from the chair - reverse the process.
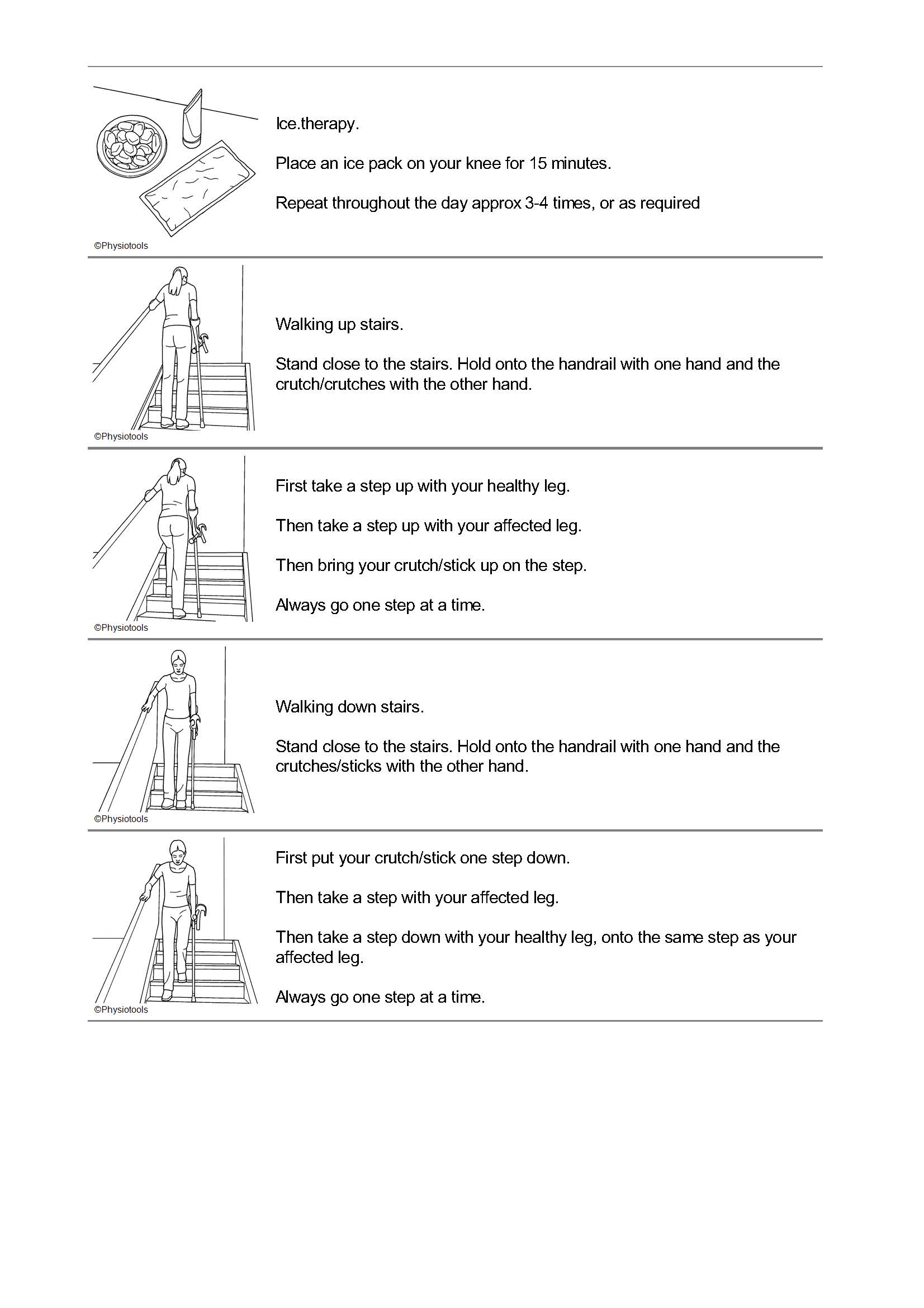
Stairs
- Always use a handrail if there is one.
- Going up - lead up with the unoperated leg, followed by the operated leg and the stick/crutch.
- Going down - lead down with the stick/crutch and the operated leg, followed by the unoperated leg.
A lot of people use this to remember – “up with the good, down with the bad”. Keep this method up until you feel strong enough to walk upstairs normally. Many patients can manage this between weeks four and six (a few stairs at a time).
Wound care
You may find that the area around your wound feels numb, tingly, itchy or slightly hard. This is normal and should disappear over the next few months. During this time you should protect it from sunlight as it will burn easily. Avoid the temptation to scratch the area until it is fully healed. You may wash around your wound with soap and water unless otherwise advised. If you have stitches or clips in your wound you will be asked to arrange an appointment with the practice nurse at your GP surgery to remove them. We will give you a letter and some clip removers (if required) to give to the nurse. If you have any concerns about your wound, please contact the ward you were discharged from.
Wound dressing
You will have an aquacel dressing over your wound which should stay in place for up to 14 days. You will be provided with a dressing to take home should you need a dressing change.
More information
Total knee replacements are performed to give patients a better quality of life, and most people are keen to return to normality as soon as possible. However, it is most important that you do not do too much too soon so as to allow healing to be as complete as possible. Hence the advice and few rules you were given on your discharge from the hospital.
Why have I still got swelling?
Healing tissues are more swollen than normal tissue. This swelling may last for several months. Ankle swelling is due to the fact that each time we take a step the calf muscles contract and help pump blood back to the heart. If you are not putting full weight on the leg, the pump is not as effective and fluid builds up around the ankle. By the end of the day lots of people complain their ankle is more swollen.
What can I do about it?
When sitting the ankle pump exercises work the calf muscles and help pump the fluid away. Try to put equal weight through each leg and “push off” from your toes on each step. Elevate the leg for 20-30 minutes regularly throughout the day and use an ice pack if you have been advised to do so by your physiotherapist.
Why is my scar warm?
Even when the scar has healed there is still healing going on deep inside. This healing process creates heat, which can be felt on the surface. This may continue for up to six months. This is a different warmth to that of an infection.
Why do I get pain lower down my leg?
The tissues take time to settle and referred pain into the shin or behind the knee is quite common.
Why do I stiffen up?
Most people notice that whilst they are moving around, they feel quite mobile. After sitting down the knee feels stiff when they stand and they need to take three to four steps before it loosens up. This is because those healing tissues are still swollen and are slower to respond than normal tissue.
Is it normal to have disturbed nights?
Yes, very few people are sleeping through the night at six weeks after the operation. As with sitting you stiffen up and the discomfort then wakes you up. You may sleep in any position that you find comfortable. If lying on your back, do not sleep with a pillow underneath your knee.
I have a numb patch - is this okay?
Numbness around the incision is due to small superficial nerves being disrupted during surgery. The patch usually gets smaller but there may be a permanent small area of numbness.
My new knee clicks occasionally – is this normal?
This can be normal and it is usually a sign that those swollen tissues are moving over each other differently than before. You should not let this worry you, as again this should improve as healing continues. If you have any concerns please speak to your surgeon.
When should I stop using a stick?
Stop using the stick when you can walk as well without it as with it. It is better to use a stick if you still have a limp so that you do not get into bad habits that are hard to lose. Limping puts extra strain on your other joints especially your back and other leg. Use the stick in the opposite hand to your operated knee. Many people take a stick out with them for three to four months after the operation as they find they limp more when they get tired.
Will I have any extra physiotherapy as an outpatient?
Everyone is referred to outpatient physiotherapy on discharge from the hospital. It is very important that you continue with the exercises you have been taught.
How far should I walk?
This varies on your fitness and what your home situation is. You should feel tired not exhausted when you get home, so gradually build up distance, remembering you have to get back.
When can I resume driving?
Always be guided by your consultant. Make sure you can reach and use the pedals without discomfort. Have a trial run without the engine on. Try out all controls and go through the emergency stop procedure. Start with short journeys and when you do a long trip stop regularly to get out and stand up and stretch. You may like to check and confirm your insurance cover.
When can I have sex?
Unless you have been advised otherwise, you should do what feels right for you. Sexual intercourse may be resumed with care when you feel comfortable. Our clinical staff are comfortable to give you advice. Please ask.
When can I fly?
You can complete a short haul flight after 6 weeks. It is recommended that you do not fly long haul for 3 months.
Will I set off the security scanner alarm at the airport?
Most joints are made of stainless steel and these may set off the alarm. If this happens have a word with security staff and explain the situation.
Will it get better?
Yes, do not despair! Do remember that most people who have knee replacement surgery have had a knee that has bothered them for a long time. Therefore it will take time to recover from surgery and your body to get used to your new knee.
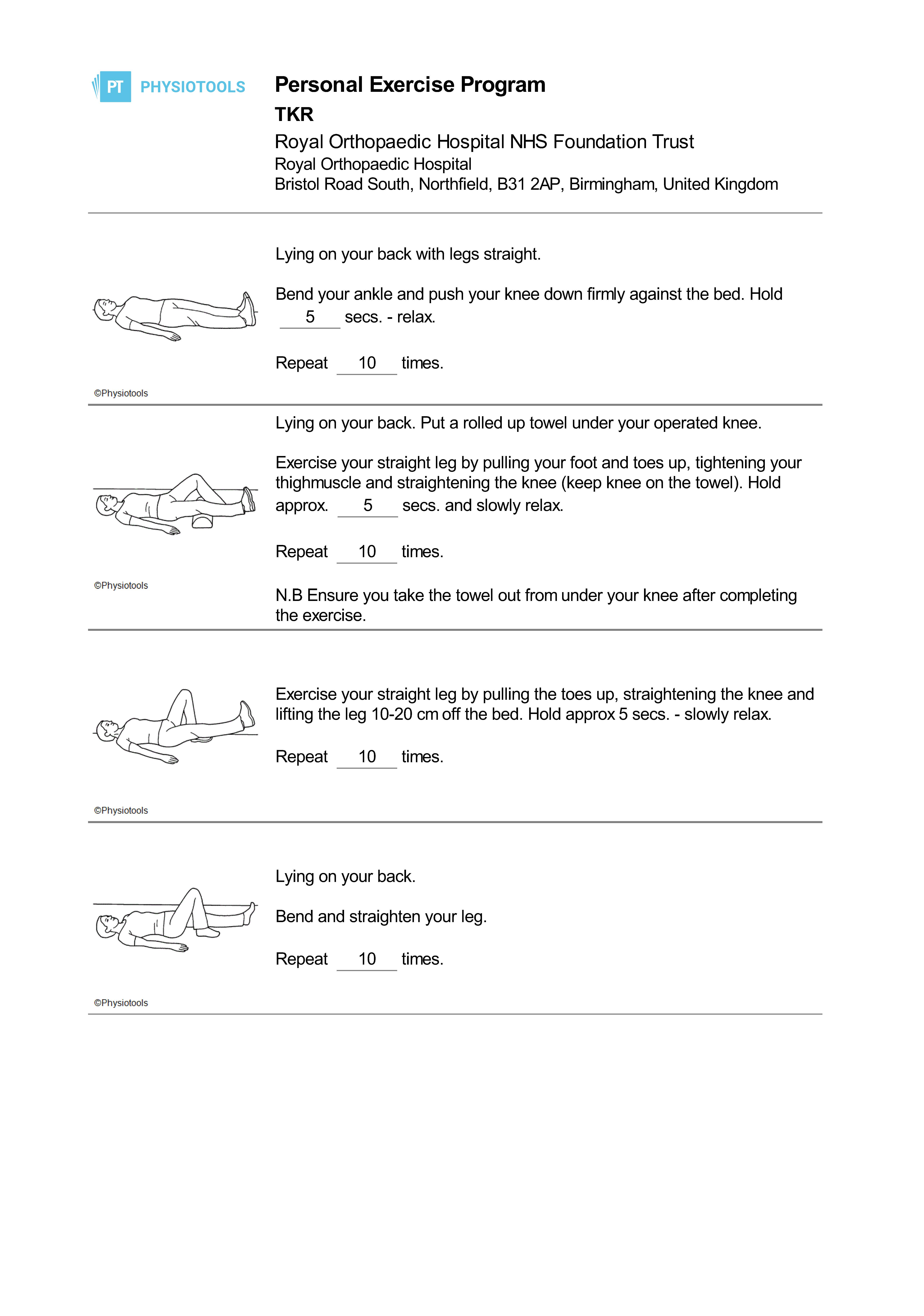
Physiotherapy